Care ABC - G for Gastritis

When the stomach rebels: What you should know and keep in mind about gastritis
Sour doesn’t always make life cheerful – especially not when there’s a real fireworks display burning in your stomach. Did you know that in the Western world, almost every second person over 50 suffers from chronic gastritis? In 80 to 90 percent of cases, the bacterium Helicobacter pylori is behind it. What makes it especially tricky: many people do not notice the disease, or only notice it very late – because the symptoms begin quietly, drag on for months, or are mistaken for other complaints.
In everyday care, inflammation of the stomach lining is an often underestimated challenge. It creeps in quietly, is confused with general loss of appetite, and affects far more than just digestion. Untreated gastritis robs people of joy in life and energy – and in weakened individuals, it also interferes with the important absorption of nutrients.
Whether you are organizing 24-hour care or are yourself lovingly caring for a family member: Knowing how to create stomach-friendly routines is worth its weight in gold. In this guide, you will learn everything about the causes, the difference between acute and chronic courses – and which small tricks in nutrition, rest, and movement really provide relief.
Because good care sometimes goes through the stomach. And sometimes it begins with a cup of chamomile tea at the right time.
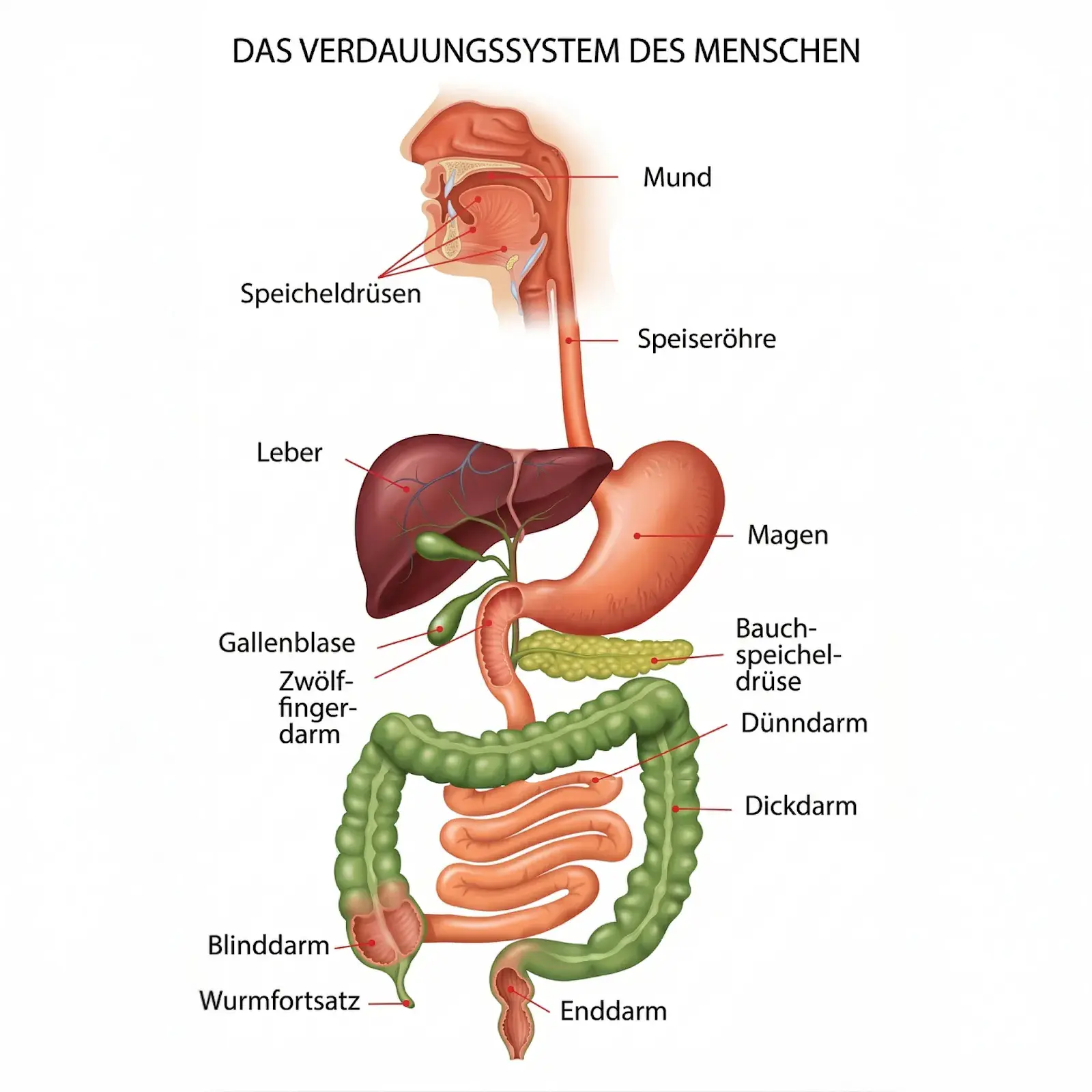
Gastritis is an inflammation of the stomach lining – that sensitive protective layer that shields the stomach wall from its own aggressive acid. If it becomes irritated or damaged, the body sends signals: stomach pain, a feeling of fullness, heartburn, nausea, loss of appetite, or vomiting. Gastritis can occur acutely – for example after a bad meal or a stressful day – or develop gradually as a chronic form that lasts for months or years.
What makes care especially challenging: Not every case of gastritis shows up with classic stomach pain. Especially in older people, it often presents much more quietly – through loss of appetite, unexplained fatigue, unclear upper abdominal discomfort, or changed eating behavior. Those who look closely can recognize these quiet signals early and act in time.
A historical look: When was gastritis discovered?
Stomach problems have accompanied people for thousands of years – but gastritis was only medically described as an independent disease in the 19th century. For a long time, it was assumed that stress, too much acid, and an unhealthy lifestyle were the main culprits.
The real turning point came in 1984. The Australian researchers Barry Marshall and Robin Warren discovered the bacterium Helicobacter pylori and demonstrated that it plays a central role in gastritis and stomach ulcers. Until then, the idea that a bacterium could survive in the highly aggressive, acidic stomach environment was considered unthinkable – and was initially met with skepticism by the scientific community. Marshall is even said to have drunk the bacterium himself to prove his theory.
Since then, it has been clear: For many chronic forms of gastritis, a bland diet alone is not enough. If Helicobacter pylori is involved, targeted eradication therapy is needed – a combination of acid-reducing medications and antibiotics.
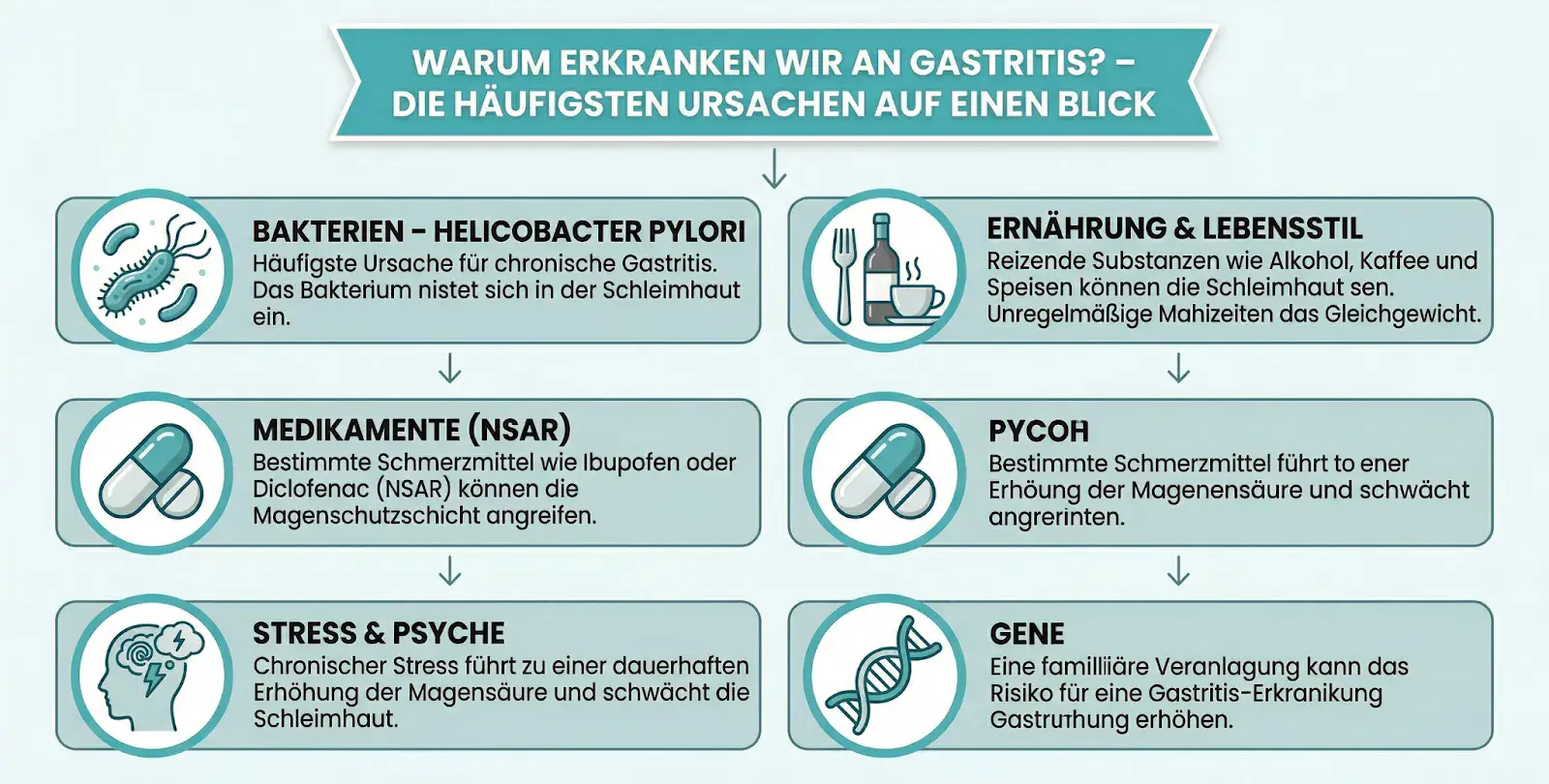
Gastritis rarely develops because of a single trigger. Most of the time, it is an interplay of several factors – diet, lifestyle, psychological stress, and genetic predisposition often work hand in hand.
The role of the microbiome
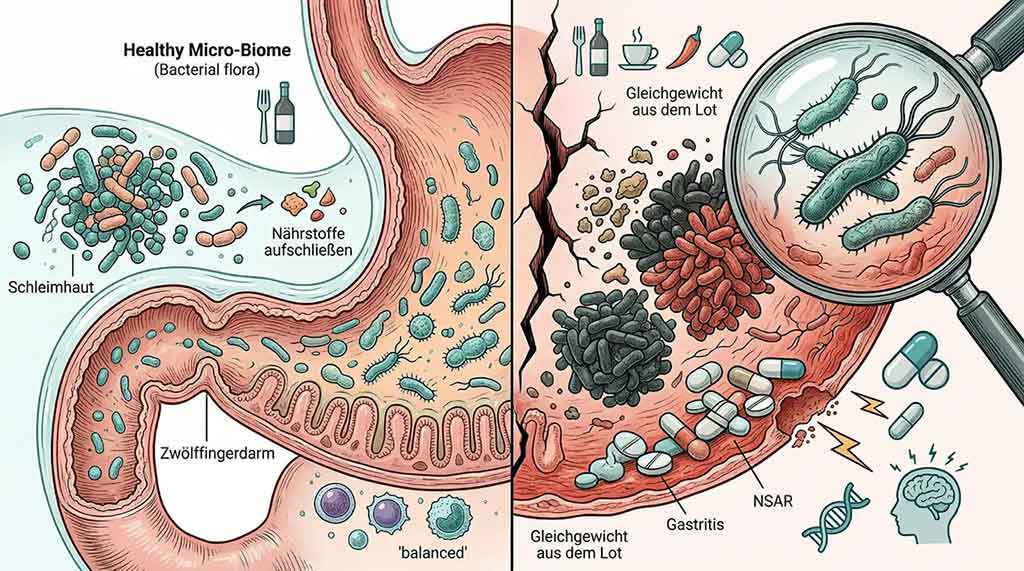
Our digestive tract is a fascinating micro-world: trillions of microorganisms – the so-called microbiome – work every day to break down nutrients, neutralize harmful substances, and keep the immune system in balance. If this balance is disturbed, the stomach lining reacts as well.
An unhealthy diet, excessive sugar consumption, alcohol, nicotine, certain painkillers (NSAIDs), and chronic stress can push back the beneficial bacteria. According to an analysis by the German Society for Gastroenterology, irregular meals, excessive coffee consumption, and lack of sleep are among the most common triggers of acute gastritis.
In everyday care, these factors are particularly relevant:
- Regular use of NSAID painkillers such as ibuprofen or diclofenac
- Irregular meals or long gaps between meals
- Very fatty, spicy, or highly acidic foods, as well as a lot of coffee or alcohol
- Persistent physical or emotional stress
- Reduced food intake in older people
- Polypharmacy and chronic comorbidities
Genetic predisposition
Our genes also play a role. Anyone who has close family members who frequently suffer from stomach problems carries an increased risk – because the predisposition affects individual acid production, the regenerative capacity of the mucosa, and the composition of the stomach flora. A conversation with your family doctor is therefore especially worthwhile when symptoms such as belching, stomach pressure, or loss of appetite keep appearing – even if they initially seem harmless.
What this means for care
Gastritis is not automatically self-inflicted. Especially in older age, several factors often come together at the same time – a body with fewer reserves reacts more sensitively to stimuli that younger people would cope with without any problem. Good care for gastritis therefore does not mean looking for blame, but rather recognizing triggers together and defusing them as much as possible.
Gastritis is not just gastritis. In everyday care, it helps a great deal to know the most important forms – because depending on the cause and course, care and treatment also differ considerably.
Acute gastritis
Acute gastritis usually starts suddenly and makes itself clearly noticeable: stomach pain, nausea, a feeling of fullness, heartburn, loss of appetite, or vomiting can occur within a few hours. Common triggers are alcohol, nicotine, strongly irritating foods, infections, stress, or certain medications. The good news: in most cases, the acute form heals completely within a few days with a bland diet, rest, and by avoiding the trigger. (Source: gesundheitsinformation.de)
Chronic gastritis
The chronic gastritis is more insidious. It develops slowly, often over months or years – and frequently remains unnoticed for a long time. Symptoms may be completely absent or so mild that they are hardly noticeable. That is exactly why it is especially relevant in everyday care: if you do not look specifically, it is easy to overlook.
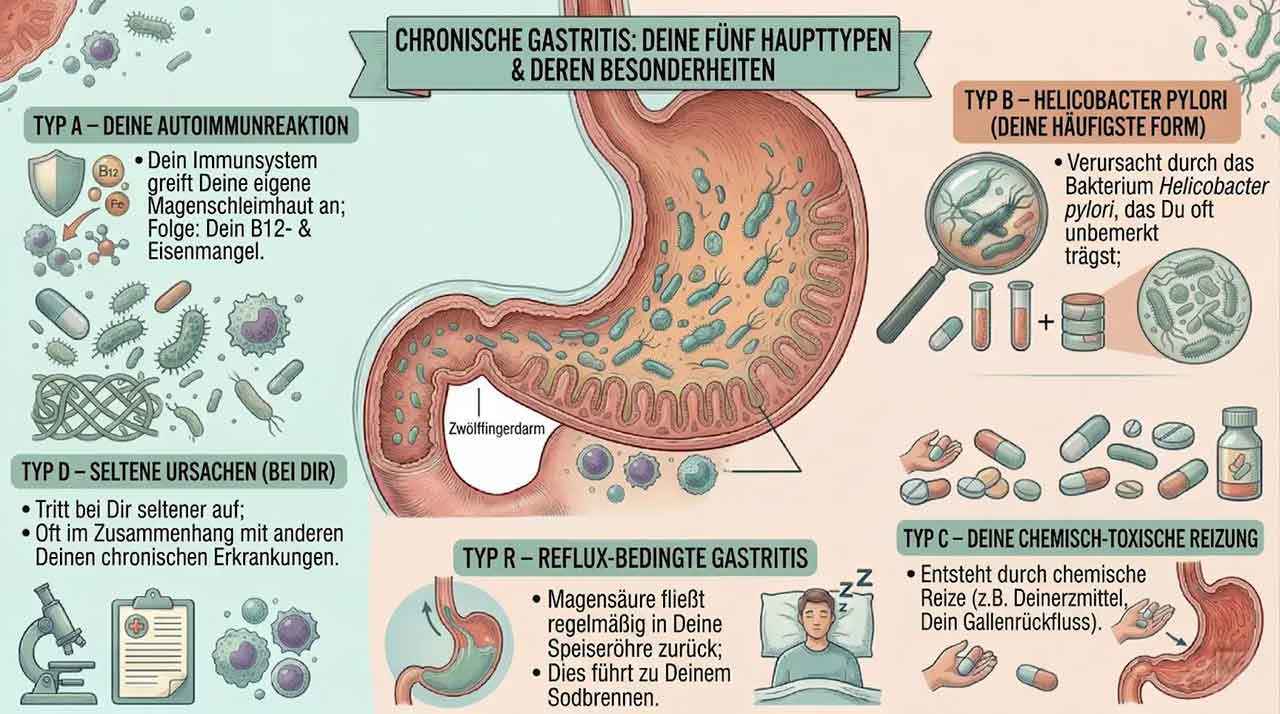
Chronic gastritis is divided into several types:
- Type A – Autoimmune reaction In Type A gastritis, the body's own immune system attacks the stomach lining. The result is often a deficiency of vitamin B12 and sometimes iron as well. This is especially tricky in older people because symptoms such as fatigue, paleness, forgetfulness, or weakness are not immediately associated with the stomach. Regular blood tests are essential in known Type A gastritis.
- Type B – Helicobacter pylori Type B is by far the most common form of chronic gastritis and in most cases is caused by the bacterium Helicobacter pylori. It settles in the stomach lining, causes permanent irritation, and if left untreated can lead to stomach ulcers. It is estimated that up to 50 percent of the world's population is infected—often without knowing it. The bacterium is detected by breath test, stool test, or gastroscopy. Treatment is carried out with eradication therapy: a targeted combination of antibiotics and a proton pump inhibitor.
- Type C – Chemical-toxic irritation Type C is caused by chemical irritation from outside—most commonly by anti-inflammatory painkillers such as ibuprofen, diclofenac, aspirin, or naproxen, but also by bile reflux. This is particularly relevant for caregivers when older people take pain medication regularly. In such cases, the medication should always be coordinated with the family doctor and, if necessary, supplemented with stomach protection.
- Type D – Rare causes Type D occurs less frequently and is often associated with other chronic inflammatory diseases such as Crohn's disease or certain infections. Close collaboration with specialists is especially important here.
- Type R – Reflux-related gastritis In reflux gastritis, stomach acid regularly flows back into the esophagus and permanently irritates the mucous membrane. Those affected know this as heartburn. A simple but effective care measure: position the upper body slightly elevated during sleep to reduce the reflux.
Gastritis does not always present the same way—and that is exactly what sometimes makes it so hard to recognize.
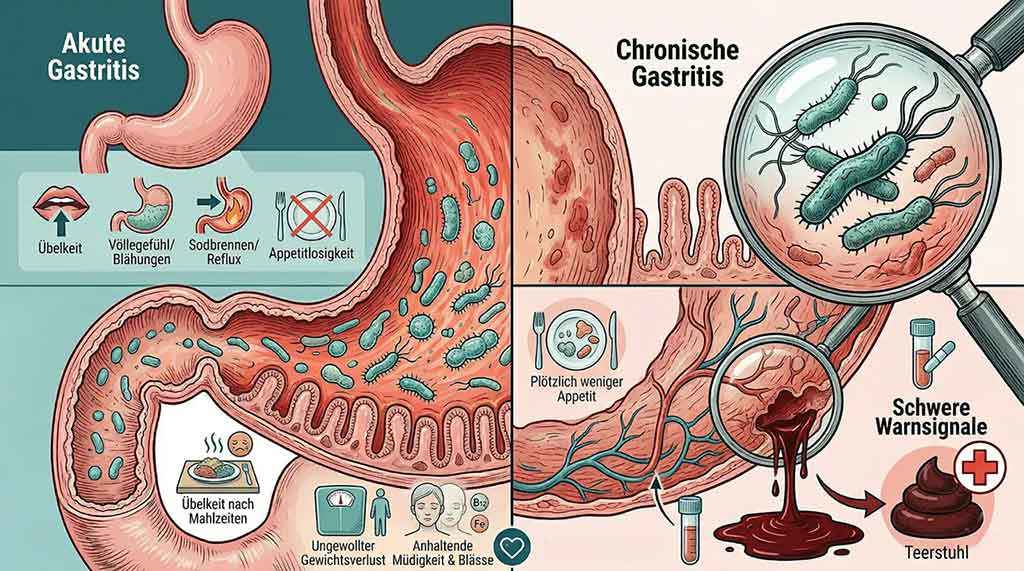
Acute gastritis usually makes itself clearly known: burning stomach pain, a feeling of fullness, bloating, heartburn, belching, nausea, or vomiting. These signs are clear and can be classified well.
Chronic gastritis is the quieter form. It can continue for months or even years without causing obvious symptoms. Especially in older or care-dependent people, it often presents very differently than expected—and is therefore often overlooked or misinterpreted.
Quiet signals you should know
Pay particular attention to these changes:
- Suddenly less appetite or aversion to certain foods
- Nausea after meals
- Unintentional weight loss without any apparent reason
- Persistent fatigue, paleness, or weakness
- Circulatory problems or dizziness
- Dark or tar-like stool—a serious warning sign of internal bleeding that requires immediate medical evaluation
Observe and document: Your mini symptom log
You do not need to keep a medical record—a simple notebook is completely sufficient. For a few days, note down the following points:
- When did pain or nausea occur—on an empty stomach or after eating?
- How severe were the symptoms on a scale of 1 to 10?
- How much did the person drink and eat?
- What was the bowel movement like—normal, dark, or tarry?
- Was there vomiting or traces of blood?
- Were medications newly started, changed, or skipped?
This information is worth gold to the family doctor and helps make the right diagnosis more quickly.
When to see a doctor immediately?
Some signs allow no delay. Seek medical help immediately for the following symptoms:
- Dark, tarry, or bloody stool
- Vomiting blood or coffee-ground-like material
- Severe, suddenly occurring upper abdominal pain
- Pronounced weakness, dizziness, or circulatory problems
- Persistent symptoms without improvement after three days
- Noticeable weight loss in a short period of time
These signs can indicate serious complications—for example, stomach bleeding or an ulcer. Here the rule is: better to see a doctor once too often than once too little.
Special features in older people
In senior citizens, gastritis is often quieter, more nonspecific—and with greater consequences if it is overlooked. These four areas deserve special attention in everyday care:

- Dehydration: Older people often have a reduced sense of thirst. With gastritis involving vomiting or loss of appetite, the risk of dehydration rises quickly. Signs include dry lips, dark urine, confusion, or dizziness. Daily fluid intake should be actively monitored—at least 1.5 liters per day is the goal.
- Malnutrition: Persistent loss of appetite can lead to measurable weight loss within just a few weeks. This is particularly dangerous in older people, as muscle loss and the risk of falls increase at the same time. Regular weighing and targeted nutritional support help detect changes early.
- Polypharmacy and NSAID risk: Many older people take several medications every day. The combination of painkillers, blood thinners, and other preparations can put considerable strain on the stomach lining. A regular review of the medication plan by the family doctor is essential—and should be actively requested in everyday care.
- Atypical symptoms: Instead of classic stomach pain, older people in need of care often show fatigue, paleness, or depressive moods —often triggered by a vitamin B12 deficiency as a result of Type A gastritis. These symptoms are easily attributed to the general aging process. Those who look closely can make the decisive difference here.
Not every stomach ache means gastritis—but anyone who has symptoms for days or weeks should take the warning signs seriously. Diagnosis is often delayed, especially in older people, because symptoms such as loss of appetite, nausea, or pressure in the upper abdomen are not immediately associated with the stomach lining.
The medical consultation
Everything always begins with a conversation. The family doctor asks specific questions: When does the pain occur—on an empty stomach or after eating? Is there nausea, belching, or vomiting? What medications are being taken? Are there any family risk factors or known stomach problems in the past?
This medical history helps establish the first connections and strengthens the suspicion of gastritis. Especially in people in need of care who cannot always express themselves clearly, it is helpful if relatives or caregivers attend the appointment and describe their observations—for example, changed eating habits, weight loss, or recurring restlessness after meals.
The gastroscopy
If the symptoms persist or recur repeatedly, a gastroscopy is recommended. It is considered the gold standard for diagnosing gastritis—and today it is much less burdensome than many fear.
During the examination, the doctor inserts a flexible tube with a small camera through the mouth and esophagus into the stomach. This allows the lining to be examined directly, and at the same time a small tissue sample can be taken. This biopsy makes it possible to determine the exact type of gastritis and to reliably detect an infection with Helicobacter pylori.
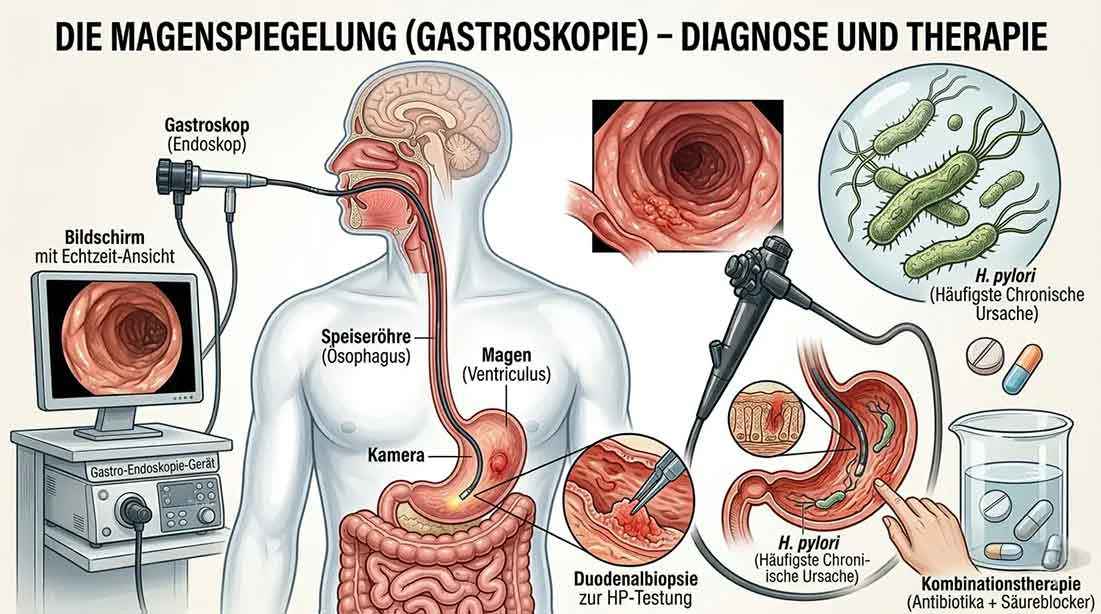
The examination usually takes only a few minutes, is largely painless, and can be performed with light sedation if desired—which can be a great relief, especially for older or anxious patients.
Further diagnostic options
Depending on the situation, gentler methods are also available:
- Breath test – The C13 breath test is the simplest method for detecting Helicobacter pylori. The person drinks a special liquid and then breathes into a tube. Non-invasive, painless, and particularly suitable for older or frail people.
- Stool test – Also non-invasive and reliable for detecting Helicobacter pylori. Can easily be carried out at home.
- Blood test – Provides information about inflammatory markers, vitamin B12 levels, and possible anemia—particularly important if Type A gastritis is suspected.
- Ultrasound – Used to rule out other causes of upper abdominal symptoms, such as gallbladder problems or liver changes.
Case example: Mrs. Huber (78) – when the stomach speaks quietly
Mrs. Huber has been living with her daughter for some time now, who lovingly takes care of her. In recent weeks, she had increasingly complained of loss of appetite and a burning pain in her abdomen—especially in the morning after getting up. At first, the family thought it was a harmless upset stomach and waited.
Only when the symptoms did not improve and Mrs. Huber noticeably lost weight did the daughter decide to visit the doctor. A gastroscopy provided clarity: chronic Type B gastritis caused by Helicobacter pylori.
For the daughter, the diagnosis meant a change in everyday life—bland food, regular medication, vitamin B12 administration, and above all patience. But the relief outweighed everything: at last the discomfort had a name. And a treatment plan.

The honest answer: It depends entirely on which form is present.
Acute gastritis: Rest, bland food, patience
The good news first: acute gastritis does in many cases actually heal on its own—provided you react quickly and give the stomach the break it needs.
The following approach has proven effective:
- Rest the stomach for one to two days – eat little or nothing, drink only still water or mild teas
- Then gradually introduce light bland foods: oat porridge, rusks, rice, or mashed potatoes
- Warmth on the abdomen, bed rest, and rest after meals
- In case of severe symptoms, antacids can help with short-term acid neutralization or proton pump inhibitors can help reduce stomach acid production – always in consultation with a doctor
Important: If the symptoms persist after three days or worsen, a doctor should definitely be consulted.
Chronic gastritis: Bland food alone is not enough here
In chronic gastritis – especially type B with Helicobacter pylori – targeted medical treatment is necessary. The bacterium does not disappear on its own and, if left untreated, can lead to stomach ulcers or long-term damage.
Treatment is carried out with what is known as eradication therapy: a combination of two antibiotics and a proton pump inhibitor over seven to 14 days. The success rate is very high when taken consistently – but that is exactly what matters. Even if symptoms subside after just a few days, the therapy must be completed in full. Stopping too early risks resistance and a relapse.
Anyone searching for care for gastritis usually wants to know one thing above all: What do I do now – today, practically, step by step? That is exactly what this section is for.
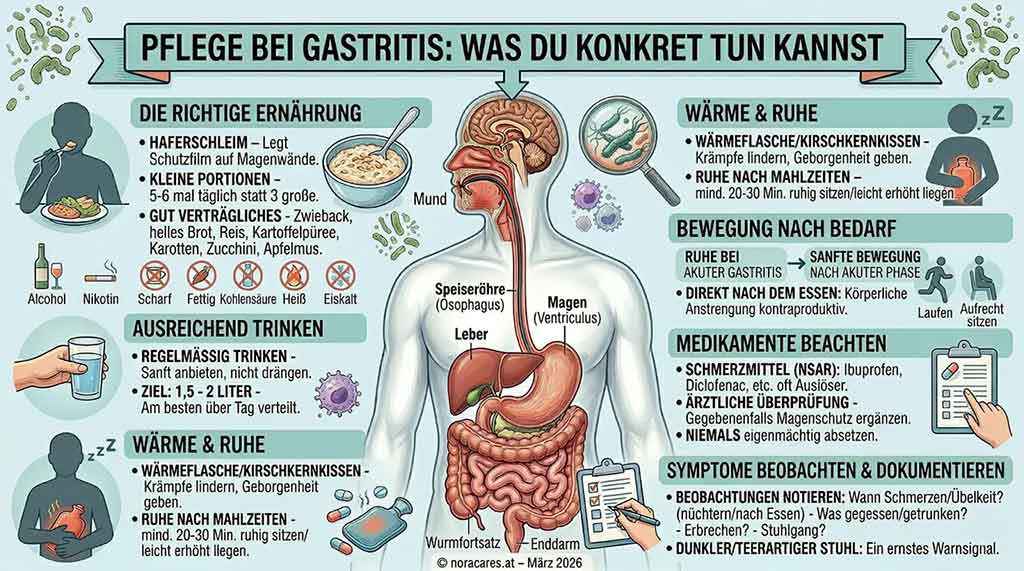
1. Relieve the stomach – with the right diet
When symptoms are acute, less is often more. Instead of two or three large meals, five to six small, well-tolerated portions spread throughout the day help – this relieves the irritated lining and gives the stomach a chance to recover.
Foods that are well tolerated with gastritis:
- Oat porridge – forms a protective layer over the stomach walls
- Rusks and white bread – mild and easy to digest
- Rice and mashed potatoes – filling without irritation
- Mild cooked vegetables such as carrots or zucchini
- Banana or applesauce – if well tolerated
- Still water and mild herbal teas such as chamomile or fennel
What irritates the mucous membrane instead: Alcohol, nicotine, large amounts of coffee, spicy or fatty foods, carbonated drinks, as well as very hot or ice-cold meals.
2. Drink enough – and provide support with it
With nausea or little appetite, fluid intake often drops unnoticed – especially in older people with a weaker sense of thirst. The goal is at least 1.5 to 2 liters daily, ideally in small amounts spread throughout the day.
A simple trick in everyday caregiving: place a small glass of water next to every plate and gently accompany drinking – do not pressure, but offer it regularly. (Source: apotheken-umschau.de )
3. Warmth and rest as gentle helpers
A hot water bottle or a cherry pit pillow on the abdomen can relieve cramps and at the same time convey comfort – which means a lot, especially for older or unsettled people.
After meals, the person in need of care should sit quietly or lie with the upper body slightly elevated for at least 20 to 30 minutes – neither get up immediately nor lie down flat. This simple habit can significantly reduce heartburn and reflux.
4. Exercise or rest – what makes sense?
The honest answer: both – but in the right amount and at the right time.
With acute gastritis involving severe pain or vomiting, the body needs rest. Physical exertion directly after eating is counterproductive.
As soon as the acute symptoms subside, gentle movement can even support recovery. A short walk after eating stimulates digestion – just 10 to 15 minutes in the fresh air have a positive effect on bowel activity and mood. Small movements indoors also help: get up slowly, walk briefly to the window, sit upright instead of lying flat.
Intense sports, heavy lifting, and pronounced bending forward directly after eating should generally be avoided with active gastritis.
5. Pay close attention to medication
Painkillers such as ibuprofen, diclofenac, aspirin, or naproxen are among the most common triggers of gastritis – and are often taken daily in caregiving routines. If symptoms occur, the medication should always be reviewed by a doctor. In many cases, a stomach-protective medication can be prescribed at the same time.
Never stop painkillers on your own – but also do not continue giving them permanently without consultation.
6. Observe and document symptoms
Good documentation is worth gold in everyday caregiving – especially for people who cannot always express themselves clearly. Note down:
- When pain or nausea occurs – on an empty stomach or after eating
- What was eaten and drunk
- Whether vomiting occurred
- What the stool looked like – pay special attention to dark or tar-like stool
- How the person appears overall – energy, mood, appetite
- Whether medications were skipped or newly started
This information helps the family doctor make the right decision more quickly.
7. When should you see a doctor immediately?
Some signs allow no delay. Act immediately with the following symptoms:
- Dark, tar-like, or bloody stool
- Vomiting blood or coffee-ground-like material
- Severe, suddenly occurring upper abdominal pain
- Pronounced weakness, dizziness, or circulatory problems
- Persistent symptoms without improvement after three days
- Significant weight loss in a short period of time
A structured daily routine helps reduce symptoms and noticeably improve quality of life.
Medicine has a lot to offer – but sometimes it is the cup of chamomile tea at the right time that makes the biggest difference. In addition to medical treatment, there are proven home remedies from traditional empirical medicine that can relieve symptoms and calm the stomach.
Many of these remedies come from traditional empirical medicine and can be taken as supportive measures alongside medical therapy – especially in the care of older people, they are a gentle addition.
Small gestures, big impact
Sometimes the best care lies in the small details of everyday life.
- Make tea times mindful: A small tea ritual with chamomile or fennel creates calm and routine – especially when it is lovingly accompanied. This is not only good for the stomach but also for the soul.
- Compote instead of pastry: A mild apple or pear compote with a pinch of cinnamon replaces heavy desserts and is gentle on the stomach – without having to sacrifice enjoyment.
- Bed by the window: The view of greenery, natural light, and fresh air positively influence emotional well-being – and this directly affects digestion and mood.
- Hot water bottle or cherry stone pillow: Gentle warmth on the abdomen relaxes cramps and provides comfort – especially for older people, a simple but effective remedy.
Sometimes your own strength is no longer enough – and that is completely okay. This decision aid shows you when home care is sufficient and when professional support becomes useful:
noracares connects you directly with experienced caregivers who not only help but truly listen – uncomplicated, transparent, and without hidden fees.

Gastritis does not only affect the stomach – it affects the whole person. Appetite, energy, mood, social participation – all of this depends on how comfortable someone feels in their own body. Especially in everyday care, where time is often limited and attention is required, an undetected gastritis can remain hidden for months.
But that is exactly the good news: those who pay attention can make a big difference. Notice changes in eating behavior early. Offer a cup of chamomile tea at the right time. Do not postpone the doctor's appointment. Check the medication list once more. These small steps are not trivial – they are real care.
Good care for gastritis does not require medical training. It requires attention, patience, and the knowledge of what matters. That is exactly what you have gained with this article.
And if you notice that you need support – whether for a few hours or long-term – noracares is there for you. On our platform, you will find qualified caregivers who not only help but truly listen. Direct, personal, and reliable.
Register now for free at noracares.at


- Antacids – Acid-neutralizing medications for short-term relief of heartburn and stomach pain.
- Eradication therapy – Treatment to completely eliminate Helicobacter pylori, consisting of two antibiotics and an acid blocker over seven to 14 days.
- Gastroscopy – Endoscopic examination of the stomach lining with tissue sampling. Considered the gold standard for diagnosing gastritis.
- Gastritis – Inflammation of the stomach lining that can be acute or chronic. Triggered by bacteria, medication, stress, or dietary habits.
- Helicobacter pylori – Bacterium that is the most common cause of chronic type B gastritis. Discovered in 1984 by Barry Marshall and Robin Warren, who received the Nobel Prize in 2005.
- Microbiome – The entirety of microorganisms in the digestive tract. A healthy microbiome protects the stomach lining and regulates the immune system.
- Proton pump inhibitors (PPI) – Group of medications that reduce stomach acid production, for example pantoprazole or omeprazole.
- Bland diet – Easily digestible nutrition with mild, low-fat, and non-irritating foods such as oatmeal, rice, crispbread, or cooked vegetables.
- Type A gastritis – Autoimmune form of gastritis in which the body forms antibodies against its own stomach lining cells. Can lead to vitamin B12 deficiency .
- Vitamin B12 deficiency – Can occur with type A gastritis and lead to anemia, exhaustion, memory problems, or neurological symptoms. Regular blood tests are important.

