Care level or degree of care Germany

Many people search for “Pflegestufe Germany” because they are in a challenging situation: a relative suddenly needs help, your own everyday life is becoming more difficult, or an application for care is coming up. Perhaps you also still have old notices with a care level, or you keep hearing the term and wonder what, if anything, still applies today.

When relatives suddenly need help, the question often comes up very quickly: care level or care grade – what actually applies in Germany? The terms sound similar, but they stand for two different systems – and that’s exactly where uncertainty begins for many families. If you’re misinformed now, you risk delays with applications or even financial disadvantages.
A quick note upfront: In Germany, there have been no care levels anymore since 2017. Today, people in need of care are classified into five care grades. This change was intended to be fairer, especially for people with dementia or psychological impairments. But what does that mean in everyday life? Which care grade corresponds to a former care level? What benefits are you entitled to? And how do you apply for the right care grade without getting lost in bureaucracy?
That’s exactly what this guide clarifies. Here you’ll find clear comparison tables, an easy explanation of care grades 1–5, practical tips for the application and the assessor appointment, as well as guidance on what you can do if the classification doesn’t fit.
If you’re currently facing a decision or simply want clarity at last: you’re not alone. This article is meant to help you gain confidence step by step.
Care level and care grade sound similar, but they refer to two very different assessment systems. While care levels focused strongly on the time required for physical care, today’s care-grade system assesses independence in everyday life – and therefore looks at the person more holistically.
What was a care level?
Care levels were the former system for classifying care needs in Germany. The basis was primarily the time required for physical assistance in everyday life.
This system had clear limits: cognitive and psychological impairments, for example in dementia, were only insufficiently taken into account. As a result, many affected people received less support than they actually needed.
What is a care grade?
The care grade is the currently valid system for classifying care needs. The decisive factor is no longer the time needed for care, but a person’s independence in daily life.
There are five care grades, which are determined using a points system. Physical, cognitive, and psychological impairments are all equally included in the assessment.
The most important difference at a glance

The care levels were like a rough grid: they sorted people into fixed categories, but often did not reflect the reality of their everyday lives. Many affected people fell between the levels, especially when their impairments were not visible. These gaps made a reform necessary.
The 2017 care reform
The 2017 care reform fundamentally renewed the system.
The legal basis was the Care Strengthening Act II, which completely replaced the care levels with care grades. The aim was to assess care needs more fairly and comprehensively – not only according to how much physical help someone needs, but according to how independently a person can still manage everyday life.
Advantages of the new system
The new care level system takes a closer look. Cognitive impairments such as dementia or disorientation are finally given equal consideration.
Instead of a few broad levels, there is now a more refined classification into five care grades that better reflect differences in everyday life.
The result: more fairness. Each person is considered as a whole – with all physical, mental, and psychological limitations. No one should fall through the cracks.
The change from care levels to care grades was not a hard cut, but rather like a smooth transition into a new system. No one was meant to suddenly be worse off or have to fight again for support. That is why the transition in 2017 was deliberately regulated automatically.
Automatic Transition in 2017 Explained
This affected all people who already had a care level at the end of 2016.
They did not have to submit a new application or fear a new assessment. The care insurance funds automatically assigned them to an appropriate care grade.
The so-called protection of vested rights applied: no one was allowed to receive fewer benefits due to the transition than before. On the contrary – many people even benefited from higher entitlements because the new system took a closer look.
You can imagine it like a move where everything is taken along: the need for care remained recognized, only the assessment became fairer and more up to date.
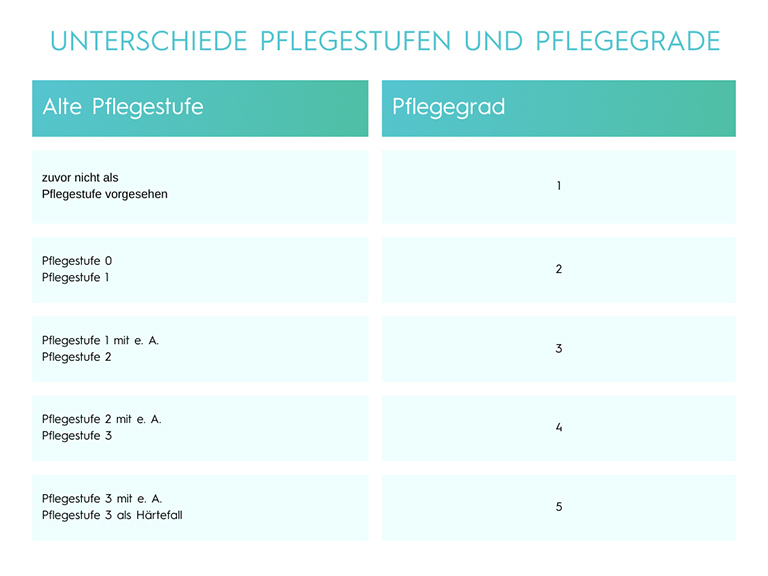
Conversion Table: Care Level to Care Grade
More than just a new name:
Let’s assume your grandma had Care Level 1 for years. She somehow managed, but it was often a struggle. Through the automatic transition, she moved into Care Grade 2.
The effect? Suddenly she not only had more money available for basic care, but also the relief amount of 125 euros. This finally allowed her to pay the everyday companion who goes for a walk with her twice a week and reads the newspaper aloud – small moments that mean the world to her and take some of the worry off you as a relative.
Special Cases in the Transition
Particular consideration was given to people with limited everyday competence. This primarily included people with dementia, but also individuals with intellectual or psychological impairments.
While in the old system they were often classified only with difficulty or not appropriately at all, during the transition they were automatically assigned a higher care grade. The new system recognized for the first time that care does not only begin where physical strength is lacking, but also where orientation, memory, or decision-making ability decline.
These special regulations in particular made the transition a noticeable step toward greater fairness for many of those affected.
Care grades indicate how severely a person’s independence in everyday life is limited – from rather mild impairments to severe support needs. The higher the care grade, the more support and benefits are available.
Care Grades 1–5 at a Glance
Care Grade 1: Mild Impairment
Care Grade 1 marks the entry into the care system. Independence is still largely present, but initial limitations make everyday life noticeably more challenging. Support here primarily serves relief and prevention.
Typical Limitations
You can still manage your everyday life largely on your own, but you need support or relief with some activities – such as shopping or organizing your day. The focus is on minor impairments of independence.
What benefits are available?
With Care Grade 1, there is no care allowance or in-kind care benefits, but you receive, for example, a relief amount for supervision and support in everyday life – such as services that make your daily routine easier.
Care Grade 2: Significant Impairment
With Care Grade 2, occasional help is no longer enough. Certain everyday activities can only be managed to a limited extent, making regular support necessary – often from relatives or a care service.
Everyday Situation
Here you are significantly more limited: tasks such as personal hygiene, nutrition, or mobility in everyday life require regular support. You can still manage many things yourself, but not without help.
Benefits
For example, you receive care allowance and/or in-kind care benefits for professional care at home. You are also entitled to short-term and respite care as well as the relief amount.
Care level 3: Severe impairment
Care level 3 stands for significantly reduced independence. Everyday life can hardly be managed without help, and many basic activities require ongoing support.
Everyday life
Your independence is severely limited. Many everyday activities, such as washing, getting dressed, or preparing food, require regular help.
Benefits
The benefits increase significantly compared to care level 2: higher care allowance, larger in-kind benefit amounts, and you can still use short-term/respite care.
Care level 4: Most severe impairment
In care level 4 the need for support is very high. Those affected depend on help in almost all areas of life – often several times a day and with close assistance.
Everyday life
Here you need intensive support with most basic everyday tasks – also spread throughout the day. This includes frequent help with personal hygiene, nutrition, and mobility.
Benefits
You receive even more care allowance and in-kind benefits than in care level 3 as well as more extensive support services, e.g., also for partial inpatient day or night care.
Care level 5: Most severe impairment with special requirements
Care level 5 describes the most intensive form of need for care. Here, in addition to the severe impairment, there are additional special requirements, for example due to complex care, complete dependency, or severe cognitive impairments.
Examples
This is the highest level: You are in very great need of care and often need support around the clock – e.g., with the most severe physical and cognitive impairments or complex care needs.
Benefits
In care level 5 you receive the highest benefits: maximum care allowance, very high in-kind care benefit amounts and comprehensive support also for special care and support tasks.
The care level is not assigned based on a feeling, but through a fixed, nationwide standardized procedure. The point is not how ill someone appears, but how independently a person can still manage everyday life. The assessment works like a close look at daily life – step by step.

Who carries out the assessment?
The assessment is carried out by an independent assessor:
- for those with statutory insurance, the Medical Service (MD)
- for those with private insurance Medicproof
The assessor usually comes to the home or to the care facility. The goal is to capture the actual everyday situation – not a “good day,” but the realistic average.
The 6 assessment modules
The assessment is carried out based on six areas of life that together provide an overall picture. You can think of them like six windows through which everyday life is viewed:
The 6 assessment modules at a glance
Important note on the calculation: In the weighting column, you can see a special feature for modules 2 and 3. The assessor evaluates both areas, but only the area with the higher score is included in the overall result at 15 percent. This prevents similar impairments from being counted twice, while at the same time ensuring that the most severe aspect (either mental performance or psychological behavior) is fully taken into account.
Example questions about the modules:
- Mobility: Can you stand up, walk, climb stairs, or move around in bed?
- Cognition & communication: Can you orient yourself, make decisions, hold conversations, and remember things?
- Behavior & psychological problems: Is there restlessness, anxiety, aggressive behavior, or nighttime disorientation?
- Self-care: Are you still able to wash, get dressed, eat, and drink independently?
- Dealing with illnesses and therapies: Can you take medication correctly, organize doctor’s appointments, or handle aids?
- Shaping everyday life & social contacts: Can you structure your day, maintain contacts, and pursue activities?
Not every module counts equally strongly – some areas carry more weight in the assessment than others. What matters is the overall picture of independence.
Points system explained
From all modules, a total score between 0 and 100 is determined.
The higher the score, the greater the impairment – and the higher the care level.
Care level thresholds at a glance:
You can imagine it like a scale: each point represents a piece of lost independence – physically, mentally, or psychologically.
Preparing for the Assessment
Good preparation can be crucial to ensure the situation is assessed realistically.
Keep a Care Diary
Over several days, note where help is needed in everyday life – even small things count.
Have Medical Reports Ready
Diagnoses, discharge summaries, or medication plans help make limitations understandable.
Avoid Typical Mistakes
Many people downplay their problems or show what they can “still manage.” What matters, however, is to describe what is regularly difficult or no longer possible – even on bad days.
The assessment is not an exam, but an evaluation of the current situation. By honestly showing your daily life, you increase the chances of receiving an appropriate and fair classification.
Your Assessment Etiquette: Confidently Through the Appointment
The assessment determines your future support. With these three golden rules, you ensure a realistic evaluation:
Assessment Etiquette
- Honesty instead of pride: Describe everyday life as it is on a bad day. Needing help is not a sign of weakness – it is the prerequisite for your entitlement.
- Support: Never attend the meeting alone. Bring a trusted person or the caring relative who can often describe the situation from an outside perspective in even greater detail.
- Care diary: Place your completed diary directly on the table as “evidence.” It shows the assessor in black and white that your need for assistance is not an isolated case, but a daily reality.
With a care level, a toolbox full of support benefits opens up. The following table shows the monthly and annual budgets.
Care allowance vs. in-kind care benefits
You can choose how you want to organize the help:
- Care allowance: When relatives or friends take over the care. The money is transferred directly to you, and you can pass it on to your helpers as a token of appreciation.
- In-kind care benefits: When a professional care service comes to your home. The service bills the health insurance fund directly.
The combined benefit (the "both-and")
Often, help from relatives is not quite enough, but a care service does not have to take over everything either. Then the combined benefit applies:
- You use part of your in-kind benefits budget for the care service (e.g., for showering in the morning).
- The remaining care allowance is paid out to you proportionally.
- Example: If the care service uses 60 percent of your in-kind benefit, you will still receive 40 percent of the care allowance.
This is how your entitlement is calculated exactly: First, the long-term care insurance fund determines what percentage of the in-kind benefits budget you have used. The percentage that remains is applied to your care allowance:

A concrete example: If you use exactly 60% of your in-kind benefit through the care service, you are still entitled to 40% of your care allowance. This keeps you flexible and ensures that no budget goes unused.
The joint annual amount (as of 2026)
In the past, respite care (replacement when relatives are on vacation/sick) and short-term care (after hospitalization) were two complicated, separate pots.
Since mid-2025, it’s simpler:
- There is a single combined pot of 3,539 euros per year.
- You can use it completely flexibly for replacement care at home or for a stay in a care facility.
- The previously required 6-month "prior care period" has been abolished – the help is available immediately from care level 2 onwards.
Additional building blocks of support
Think of these benefits like the “Swiss Army knives” of care: they are not for direct nursing care, but they solve the many small problems that often make life at home complicated. While cash and in-kind benefits form the foundation, these building blocks ensure everyday life remains safe, the home adapts, and caregiving relatives do not burn out.
The relief amount (€125)
This amount is a reimbursement. You pay for a service (e.g., cleaning help, everyday companion, shopping assistance) and submit the invoice to the fund.
- Important: In care level 1, this amount can also be used for personal care provided by a care service.
- Tip: Unused amounts are carried over to the next month. Whatever you still have left at the end of the year, you can use until June 30 of the following year.
Emergency call system & aids
- Emergency call system: From care level 1 the fund pays a monthly subsidy (usually around 25.50 euros) toward renting an emergency call system.
- Care aids for consumption: 40 euros per month for gloves, bed protection pads, and disinfectant. You can often simply subscribe to these as a package from pharmacies or medical supply stores.
- Technical aids: Care beds or lifting hoists are almost fully covered with a prescription/application (small co-payment of max. 25 euros).
Home adaptation
If the bathroom needs to be rebuilt to be barrier-free or a stairlift is required, the fund contributes up to 4,000 euros. This applies already from care level 1! If two people in need of care live together, this amount can even increase to up to 16,000 euros.
Useful information for relatives
Anyone who cares for someone at home (at least 10 hours/week spread over 2 days) is covered through the long-term care insurance fund for pension, accident, and unemployment insurance. The fund therefore pays contributions toward your pension while you provide care – an important building block for your own security.
Getting the ball rolling often takes some overcoming, but it is the most important step toward relief. Applying for a care level is not a bureaucratic obstacle course, but a structured process. You can think of it like registering for an inventory check: the earlier you submit the application, the earlier the financial security is in place, because the benefits are paid retroactively from the month in which the application is submitted.
Submit the application
The first step is the simplest – an informal sentence is enough.
- Where: The application is submitted to the long-term care insurance fund. This is always affiliated with the health insurance fund. So you simply contact your usual health insurance fund.
- How:
- Informal: A phone call, an email, or a short three-line letter by post (“I hereby apply for long-term care insurance benefits for [Name]”) is sufficient.
- Digital: Most funds now offer an app or an online portal through which the application can be submitted with just a few clicks.
- Form: After your informal contact, the fund will send you a detailed form. Fill it out carefully and send it back.
- Important: The date of the first contact counts as the application date!
Process after submitting the application
As soon as the application has been received, an automated process starts.
- Appointment scheduling: The long-term care insurance fund commissions the Medical Service (MD) (for those with statutory insurance) or Medicproof (for those with private insurance). An assessor will contact you to arrange an appointment for the home visit.
- The assessment: The assessor comes to your home (or to the facility). In about 60 to 90 minutes, they assess your independence based on the 6 modules. This is not about medical diagnoses, but rather: “What can you still do on your own and where do you need help?”
- The decision notice: The assessor sends their recommendation to the long-term care insurance fund. The fund makes the final decision and sends you the written decision notice by post. This letter states your care level and the assessment score.
Duration & deadlines
So that those affected do not have to wait months for help, there are strict statutory time requirements.
- The 25-working-day deadline: From the day your application is received by the fund, it has 25 working days to deliver a written decision notice to you.
- Delay payment: If the long-term care insurance fund does not meet this deadline (without you being responsible for the delay, e.g., by canceling appointments), it must pay you €70 for each week of the delay that has begun.
- Urgent cases: If the applicant is in hospital or a hospice, the deadline for the assessment is often shortened to one week so that care is secured immediately after discharge.
- Objection: If you do not agree with the result, you have one month after receiving the decision notice to file a written objection.
Sometimes the assessment result does not match everyday reality as experienced: the care level is too low or the application was rejected entirely. This is no reason to resign, but a moment for a “second look”.
Since assessors are only human and evaluate a snapshot in time, the law provides clear ways to bring about a correction. You can think of it like a revision in which missing details are submitted afterward to complete the picture.
File an objection
When the decision notice arrives and the classification does not appear correct, an objection is the right tool.
- Deadline: You have exactly one month after receiving the decision notice. The postmark date counts.
- Process:
- Step 1: Informal objection. First send a short letter to the long-term care insurance fund: “I hereby lodge an objection to the decision notice dated [date]. A detailed justification will follow.” This preserves the deadline.
- Step 2: Request the assessment report. At the same time, request the detailed assessment report from the Medical Service (MD) if it was not enclosed. Only then will you see in which module the assessor “forgot” points.
- Step 3: Write the justification. Compare the assessment report with your care diary. Write down which limitations are missing from the report or were assessed incorrectly.
- Step 4: Second assessment. The fund then often sends another assessor for a second assessment (objection assessment).
Apply for a higher care level
A care level is not set in stone. Since many illnesses (such as dementia or Parkinson’s) progress, the need can change at any time.
- When does it make sense?
- If your health condition has deteriorated significantly (e.g., after a fall, stroke, or with increasing immobility).
- If the previous benefits are no longer sufficient to ensure care.
- If at least six months have passed since the last assessment (in cases of acute deterioration, it can be sooner).
- The process: An application for a higher classification works exactly like the initial application. You contact the fund and say: “The need for care has increased; I am applying for a higher classification.” A new visit by the assessor follows.
- Tip: Document the new limitations for about two weeks in a care diary before applying, to be able to demonstrate the increased effort.

Care does not always take place in a wheelchair. Often it is the “quiet” limitations that place the greatest burden on everyday life. While you can see a broken leg immediately, psychological scars or the slow fading of memory are different.
In these special cases, the care level functions like a protective shield that provides support where inner strength wanes or a child’s development requires special attention.
Care level for dementia
Dementia is the classic case of “invisible” care. Physically, those affected are often still fit, but the ability to manage everyday life is lost.
- The focus: Here, the assessor looks especially into the windows of cognition (Module 2) and behavior (Module 3).
- The challenge: It’s not about whether someone can wash themselves, but whether they know they have to do it and can still plan the necessary steps.
- Special feature: Because people with dementia often maintain a “facade” and can suddenly seem very clear during the assessor’s visit, the care diary kept by relatives is vital here to document nighttime restlessness or disorientation.
Care grade for children
For children, the assessment is a comparison with peers. Every child needs help – a baby has to be changed, a toddler needs help eating. That is normal.
- The benchmark: A care grade is only assigned if the need for help significantly exceeds what a healthy child of the same age would require.
- Special feature for babies (0–18 months): Since all babies are dependent in self-care, they are automatically classified one care grade higher to better cushion the parents’ enormous care workload.
- Assessor: For children, specialized assessors usually come, who have a trained eye for child development.
Mental illnesses
Severe depression, schizophrenia, or anxiety disorders can make someone just as in need of care as physical paralysis.
- Motivation and structure: If the mental strength is missing to get up in the morning, carry out personal hygiene, or maintain social contacts, independence drops massively.
- Module focus: Here, the main focus is on organizing everyday life (Module 6) and psychological problem situations (Module 3).
- Important: Those affected often feel ashamed during the assessment and try to appear “normal.” Here it is important to honestly describe that the illness acts like an invisible barrier that can make even the simplest tasks impossible.
Even if the terms sound similar, the systems in Germany and Austria follow different logics. While Germany classifies into care grades (1–5) and measures independence, Austria uses care allowance levels (1–7), which are primarily calculated according to the amount of care time per month.
Anyone who lives in Austria or moves there must submit the application to the responsible insurance carrier (usually the PV).
For detailed information about the Austrian system and local support, we recommend our separate article “Care levels 1–7 in Austria: Benefits and care allowance at a glance”.

The question “care level or care grade?” may still leave you feeling uncertain to this day – especially when care suddenly becomes necessary and you have to make quick decisions. Important for you to know: care levels are a thing of the past. Today, there are five care grades, which reflect how independently you can still manage your everyday life and fully take cognitive limitations into account as well.
Whether you are only just considering submitting an application, want to classify an earlier care level, or are checking whether your current care grade still fits: being well prepared makes a real difference for you. If you understand how the assessment works, gather your documents, and know which benefits you are entitled to, you increase your chances of a fair classification – and ease your own burden in an already challenging situation.
Take the time to go through the individual care grades and the benefit overviews at your leisure. Use the checklists in this guide, prepare specifically for the appointment with the assessor, and don’t hesitate to file an objection if you have doubts. Seeking help is not a sign of weakness – it is your most important step to get the best possible support for yourself or your relatives.
Care is never just a bureaucratic question; it affects you, your family, and your quality of life. This guide is intended to give you orientation and convey a sense of security. If you now know which system applies, what you are entitled to, and what your next step looks like, you have already gained the most important thing: clarity.


- Application date: The day on which the care insurance fund is contacted for the first time (even informally). It is crucial because benefits are paid retroactively from that month.
- Protection of existing rights: A legal guarantee from the 2017 reform. It ensures that no one who already had a care level is worse off due to the switch to the care grade system.
- Relief amount: A budget of 125 euros per month (for all care grades) that can be used for everyday support (e.g., cleaning help, shopping service) for a specific purpose.
- Combined annual amount: A flexible pot of 3,539 euros per year (as of 2026), which can be used for short-term care and respite care.
- Personal emergency response system: A technical system that allows people in need of care to call for help at the push of a button. The fund often pays a monthly subsidy for this.
- Application for a higher classification: A new application if the health condition has worsened and the current care grade is no longer sufficient.
- Combined benefit: A mixed form of care. Professional benefits in kind and private care allowance are combined proportionally.
- Medicproof: The medical service of private health insurers. It conducts the assessment for people with private insurance.
- Medical Service (MD): The assessment service of the statutory health insurance funds. It checks on site how independent the applicant still is.
- Modules (assessment): The six areas of life (e.g., mobility, self-care) that the assessor reviews to evaluate the need for care.
- NBA (New Assessment Assessment): The scoring system (0–100 points) used to determine the level of independence.
- Care allowance: A cash benefit for people in need of care (from CG 2) who are cared for at home by relatives or friends.
- Care grade: The classification system in force since 2017 (grades 1 to 5). The determining factor here is the impairment of independence.
- Disposable care aids: Products such as disposable gloves or disinfectant for which the fund reimburses 40 euros per month.
- Benefits in kind: A budget for using a professional outpatient care service.
- Care level: The outdated system (until 2016) that primarily measured the need for care by the time required for physical help (“minutes of care”).
- Care diary: A private documentation by relatives to show the assessor exactly where help is needed in everyday life.
- PSG II: Long-Term Care Strengthening Act II (the basis of the 2017 reform).
- Independence: The central criterion of the current care system. The question is: “What can the person still do on their own?” instead of “How ill are they?”.
- Respite care: Substitute care when the main caregiver (e.g., due to vacation or illness) is unavailable.
- Objection: A legal remedy against a decision by the care insurance fund. After receiving the decision, you have one month to request a correction of the classification.
- Home adaptation: Subsidies of up to 4,000 euros for conversion measures (e.g., barrier-free shower or stairlift) to make it possible to continue living at home.

